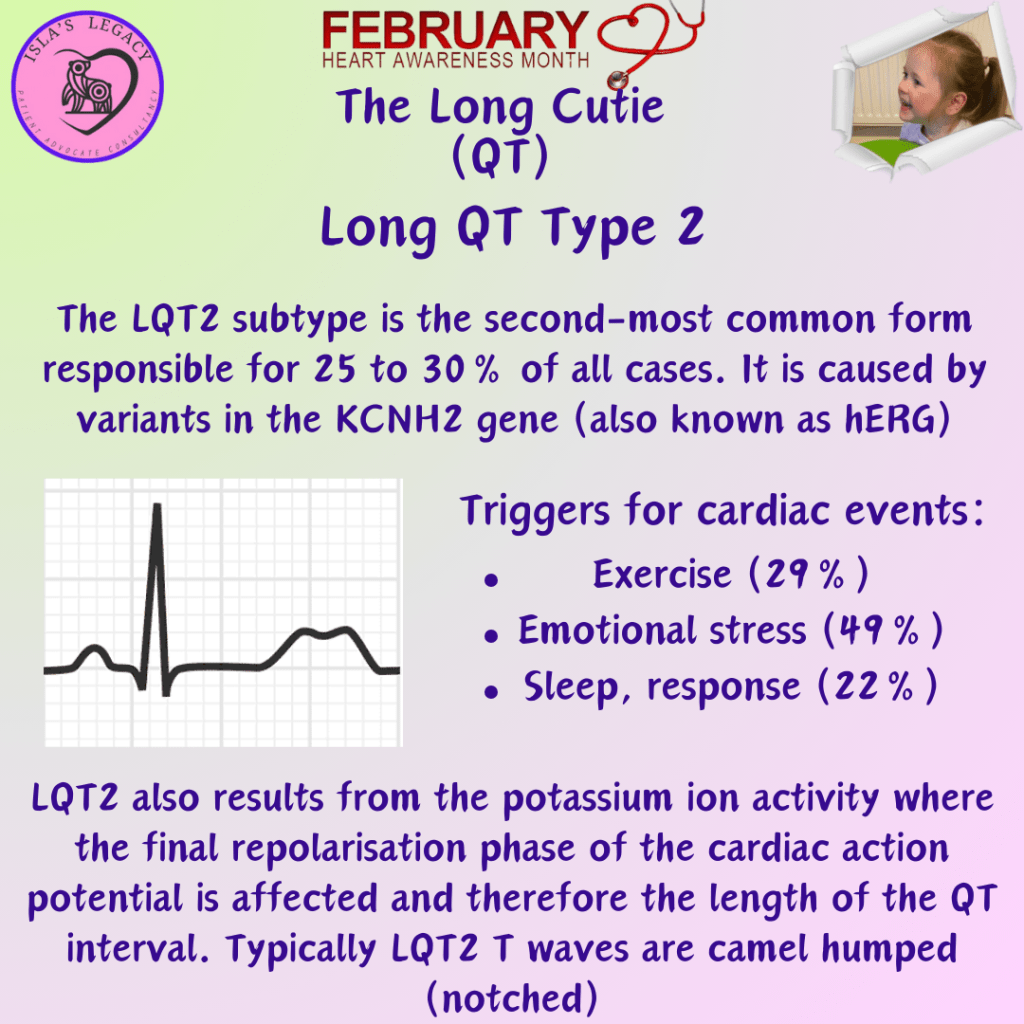
Patients with LQT2 tend to present ventricular arrhythmia in response to emotional stress (49%) or sudden auditory stimuli (eg, an alarm-clock), and less frequently during sleep (22%) or exercise (29%). Up to 20% of cases can have a nondiagnostic ECG before stimuli.
The clinical presentation of LQT2 is distinguishable from other types of LQTS by the fact that episodes of torsades de pointes (TdP) are often stimulated by the sudden sympathetic ‘fight or flight’ stimulation I.e. ‘you almost gave me a heart attack!’ response to a surprise (they mean cardiac arrest). Unfortunately for women with LQT2 the postpartum hormones (prolactin and oxytocin) have been found to increase the risk of QT prolongation and therefore adverse cardiac events in postpartum women with LQT2 (Credit: futuremedicine.com)
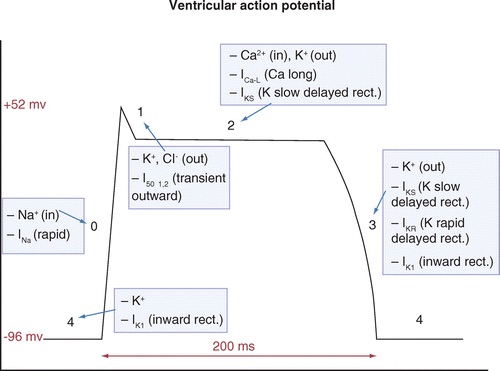
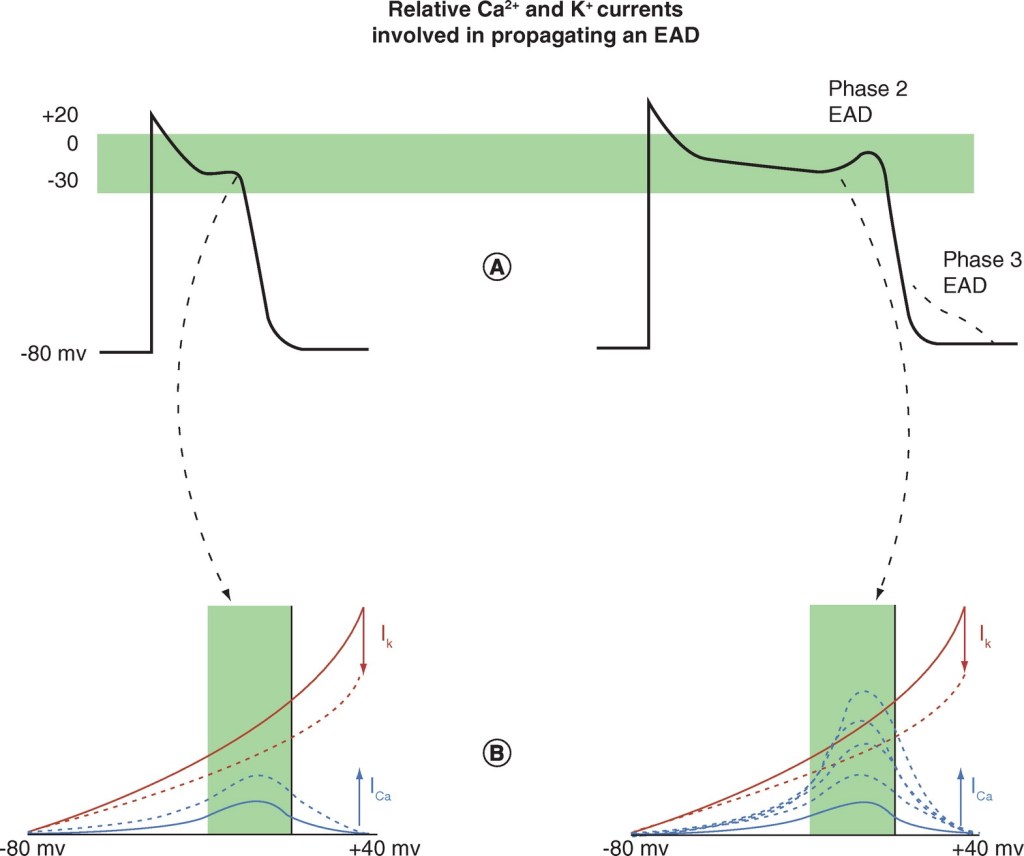
In LQT2, the QT interval is prolonged as a result of the mutated hERG channel where Phase III IKr K+ (potassium) takes longer (see picture 2). As the influx of the Ca2 (calcium) current from Phase II is greater than the relative potassium current in Phase III going out, it is enough to reverse the repolarisation of the heart cell and cause an early afterdepolarisation (see picture 3).
An early afterdepolarisation (EAD) is simply the reversal or delay of the repolarisation process and can result in ectopic beats. So essentially, for a split second the heart’s relaxing phase restarts midway through its relaxing phase… if that’s makes sense!