
Ezra was diagnosed with Long QT 1 very early through genetic testing with the mutation passed down through the paternal side. Fortunately, this has meant that Ezra has been under the protection of beta blockers all his life. While Ezra hasn’t had any confirmed cardiac events, he has had 2 syncope episodes while unwell with a fever, which could be Torsades related but also could simply be virus related fainting episodes. The doctors at the local dismissed it being heart related completely, something which I take issue with. Ezra has an AED (provided by the Oliver King Foundation who recently successfully campaigned for all schools in England to have access to defibrillators) so he is lucky to have this added level of protection.

Ezra is generally a healthy little boy and is extremely happy. At 2 years old he acknowledges the importance of his heart medicine and is very compliant taking his beta blocker himself morning and night. However, there have been multiple instances over the year that highlight how much more work needs doing to raise awareness of Long QT Syndrome and the need for improved therapies. This patient story is probably more of a rant than a patient story but Ezra’s story shows there has been little to no progress over the last 8 years.

Firstly, beta blockers. Beta Blockers are still the first line of defence for people with Long QT Syndrome. Many people suffer debilitating side effects from beta blockers such as extreme tiredness, weight gain, depression, shortness of breath. Ezra is happy taking his beta blocker, atenolol, but does feel its effects whether he realises it or not.

Cold hands or feet are a common side effect of beta blockers and something which certainly affect him. Ezra has been under respiratory care since he was born; one of the common side effects of atenolol is wheezing, coughs, shortness of breath/trouble breathing. As a wild 2-year-old, with a developing respiratory system, Ezra is often sick as a result of excessive coughing after running around. Beta blockers are vital for his heart but obviously causing other issues.
Medications to alleviate the wheezing are contraindicated (see point 2).
Another underacknowledged problem with beta blockers is their effect on melatonin production. While it is common that 2 year olds don’t sleep (I am sure every parent of a toddler is nodding right now), beta blockers can decrease the amount of melatonin by up to 80% via inhibition of the adrenergic beta1- receptors. It is therefore recommended that patients on beta blockers take a melatonin supplement in the evening, something I know is not routine and a response back to ‘he has trouble sleeping’ was ‘maybe he’s just not a sleeper’. As a patient advocate, I don’t see this as an acceptable response.

Secondly, QT prolonging medications. Most toddlers will at some point be admitted to hospital with breathing difficulties and require support breathing due to a RSV (respiratory syncytial virus) like bronchiolitis. This was an issue Isla had. I vividly remember a doctor telling me that Isla being unable to have salbutamol was ‘extremely inconvenient’. The alternative ‘safer’ medication they gave her via nebuliser, Atrovent, I got stopped extremely quickly. I was the one monitoring her ecg, not supervised by a doctor as ‘it would be fine’, prevented her from having a cardiac arrest by immediately pulling it away from her. I was lucky that a consultant who trusted my knowledge admonished the registrar who tried to dismiss my observations. Saline nebulisers were our only choice. This was 5 years ago. Ezra proves that nothing has changed.
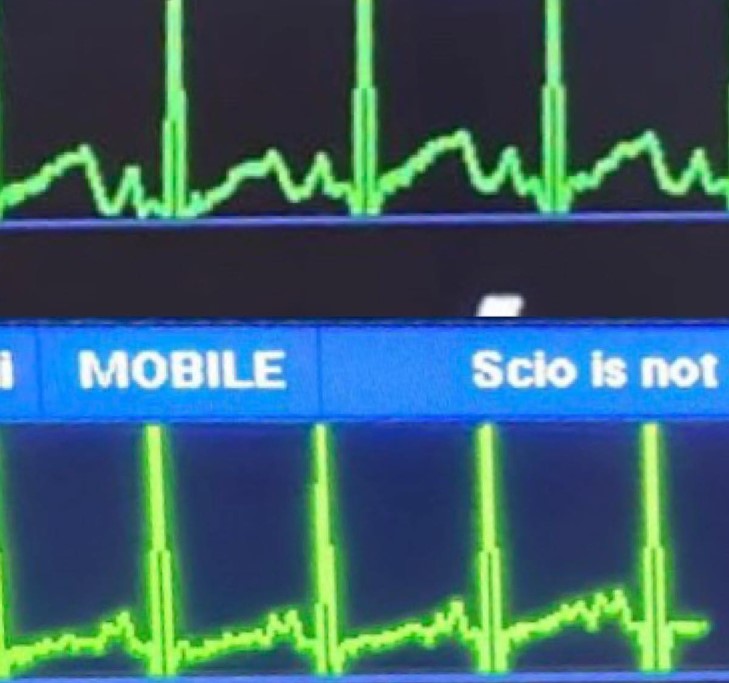

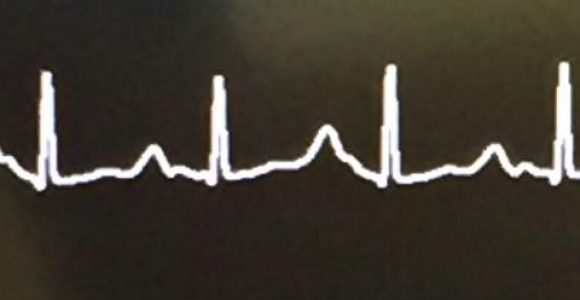
Struggling to breathe, with a Long QT diagnosis, doctors prescribed salbutamol nebulisers 4 times a day. I monitored his ecg via Facetime and I was terrified of what I saw. When I explained to the doctor over the phone that what they were doing was unsafe, the response was, ‘he’s had it once and was ok so he’ll be fine’. When pointed out that it may not be ok next time, I was told that there was no one qualified on the ward to read his ecg during salbutamol administration. No one qualified to tell if sinus rhythm, albeit with a prolonged QT interval, goes into a wiggly arrhythmia? Ok… I’m fairly certain I could train monkeys to make that distinction.

Finally, knowledge. During the hospital stay I talked about above, a nurse explained to a student nurse when she asked what Long QT is, that ‘Long QT is just a fast heartbeat’. I have no problem with nurses not knowing every condition in the human body, especially on the children’s ward of a general hospital, but if you don’t know the answer, say ‘I don’t know, lets go and look it up!’
The other lack of knowledge incident happened only weeks ago. ‘Long QT? Can you spell it for me?’ For real. This was from a medical professional. It shows there’s still a lot of work to do.
Abby (Ezra’s mum) was worried that because Ezra had had nothing major happen to him with his Long QT Syndrome, there would be no story to tell. I think Ezra’s journey so far is a story in itself as it encapsulates many of the struggles Long QT patients face. Plus, how can anyone not want to read about the boy with these curls and that smile!

